
In September 2025, the Office of Inspector General (OIG) rang the alarm bell on MDS coding inaccuracies involving falls with major injury, and the Centers for Medicare & Medicaid Services (CMS) took actions that every director of nursing services (DNS) needs to understand from an MDS perspective to be more proactive from a quality perspective, points out Angie Szumlinski, LNHA, RN-BC, GERO-BC, RAC-CT, BS, director of risk management for HealthCap/QA Reader in Ann Arbor, MI.
“The OIG identified serious discrepancies between falls with major injury reported in MDS item J1900C (Number of Falls Since Admission/Entry or Re-entry or Prior Assessment (OBRA or Scheduled PPS), Whichever Is More Recent: Major Injury) and falls with major injury reported in hospital claims data for residents who were sent to the hospital,” explains Szumlinski. “The OIG laid out its case in the report Nursing Homes Failed to Report 43 Percent of Falls With Major Injury and Hospitalization Among Their Medicare-Enrolled Residents and the data snapshot Serious Falls Resulting in Hospitalization Among Medicare-Enrolled Nursing Home Residents, July 2022–June 2023.”
Almost concurrently, CMS took steps to revise the falls definitions and coding instructions in the Long-Term Care Facility Resident Assessment Instrument 3.0 User’s Manual (RAI User’s Manual) effective Oct. 1, 2025, says Szumlinski. “For MDS coding purposes, the definitions of a fall and a major injury are broader now than they were prior to Oct. 1, 2025. CMS’s goal appears to be to align the definitions so that nursing homes can reduce under-reporting on the MDS and improve the accuracy of quality measure (QM) reporting.”
These changes covered MDS items J1700 (Fall History on Admission/Entry or Re-entry), J1800 (Any Falls Since Admission/Entry or Re-entry or Prior Assessment (OBRA or Scheduled PPS), Whichever Is More Recent), and J1900 (Number of Falls Since Admission/Entry or Re-entry or Prior Assessment (OBRA or Scheduled PPS), Whichever Is More Recent). Note: For information about the revisions, listen to the HealthCap podcast Heart-to-Heart With HealthCap: Ep 36: Inside the 2025 MDS Updates With Jane Schoof: What Clinicians Need to Know and review the Jan. 12, 2026 AAPACN article “Major Changes on Falls With Major Injury QMs.”
Why these coding changes matter to the DNS
Failing to incorporate the Oct. 1, 2025 changes to accurately code falls on the MDS could have repercussions for several QMs, in particular the long-stay QM Percent of Residents Experiencing One or More Falls With Major Injury (Long-Stay) and its short-stay sibling Application of Percent of Residents Experiencing One or More Falls With Major Injury (Long-Stay), says Joel VanEaton, BSN, RN, RAC-MTA, RAC-MT, RAC-CTA, RAC-CT, executive vice president of post-acute care regulatory affairs and education for Broad River Rehab in Asheville, NC.
“One or the other of these two measures currently affects—or will soon affect—the three federal quality programs that nursing homes participate in,” explains VanEaton. “That includes the Nursing Home Quality Initiative (NHQI) and the Five-Star Quality Rating System, the Skilled Nursing Facility Quality Reporting Program (SNF QRP), and the Skilled Nursing Facility Value-Based Purchasing program (SNF VBP).”
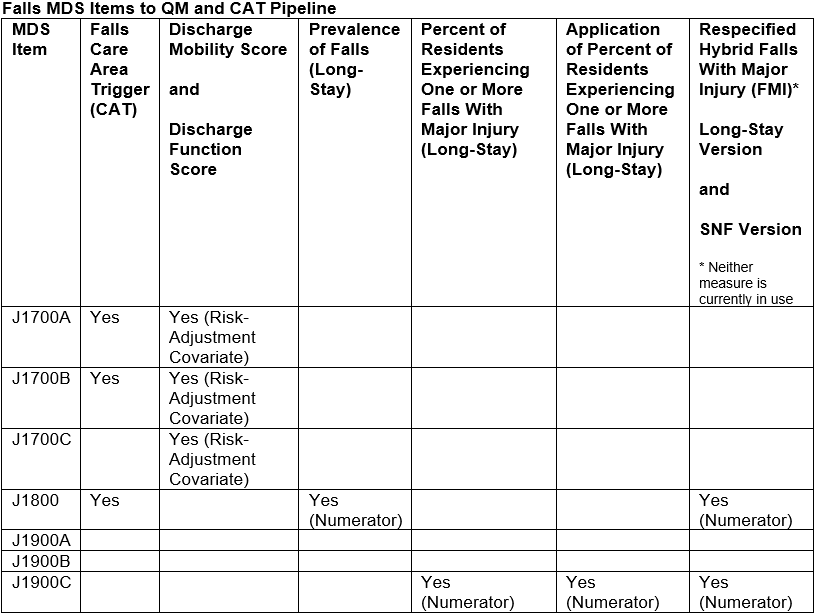
Note: For details on how falls MDS items flow into the QMs and other CMS requirements, see the AAPACN chart “Falls MDS Items to QM and CAT Pipeline” at the end of this article. For information on how QMs that use falls MDS data then feed into federal quality programs for nursing homes, see the AAPACN chart “Solve the Puzzle: How QMs Using Falls MDS Data Fit Into SNF QRP, SNF VBP, and NHQI/Five-Star,” also at the end of this article.
“Moving forward, nursing homes should expect CMS to announce a timeline for the replacement of both Falls With Major Injury (FMI) measures—most likely sometime this year (i.e., 2026),” says VanEaton. “Like the recently respecified NHQI/Five-Star QM Percent of Residents Who Received an Antipsychotic Medication (Long-Stay), the respecified FMI measures will be hybrid measures that are generated using claims data, as well as MDS data, to improve QM accuracy.”
Essentially, the respecifications provide CMS with a process to cross-check falls MDS coding against relevant ICD-10-CM diagnosis codes on hospital inpatient, observation, and emergency department claims or encounters within the QM calculations, points out VanEaton. “These changes will significantly reduce the chances of a fall with major injury going unreported in any nursing home’s QMs for NHQI/Five-Star, the SNF QRP, or the SNF VBP (while also giving CMS the ability to more easily identify providers that may have a trend of MDS undercoding instead of isolated miscoding).”
In the SNF VBP, for example, inaccurate MDS coding may result in a facility having an inaccurate incentive adjustment factor or multiplier, notes VanEaton. “That could impact how much of the 2 percent SNF VBP payment reduction your facility gets back starting this coming fiscal year (FY) 2027 (Oct. 1, 2026 – Sept. 30, 2027) with the addition of the current FMI measure and the Discharge Function Score to the SNF VBP measure set.”
Further, the MDS data that nursing homes are submitting in the current FY 2026 (Oct. 1, 2025 – Sept. 30, 2026) will have implications in the SNF VBP for several years to come, stresses VanEaton. “FY 2026 MDS data will count toward your FY 2028 (Oct. 1, 2027 – Sept. 30, 2028) performance period and your FY 2030 (Oct. 1, 2029 – Sept. 30, 2030) baseline period for your FMI and Discharge Function Score measures. So, the falls data collected using those updated definitions—and the always difficult section GG (Functional Abilities) coding—really needs to be accurate.”
Note: CMS explains the respecified FMI measures in the Long-Stay Nursing Home—Falls With Major Injury Respecification Technical Specification Report, the Skilled Nursing Facility—Falls With Major Injury Respecification Technical Specification Report, and (for the SNF QRP version) the Web-based training course Falls With Major Injury (FMI) Quality Measure (QM) Respecification. The training course includes a detailed walkthrough of coding examples related to the Oct. 1, 2025 revisions.
Taking the following steps may help the DNS work with the nurse assessment coordinator (NAC) and the interdisciplinary team (IDT) to boost alignment between accurately coded MDS assessments and fall prevention in the nursing home, according to Szumlinski:
Ensure that nursing and therapy are documenting falls appropriately
“Many nursing homes incorporated the RAI User’s Manual definition changes into their falls policy, says Szumlinski. “However, the education piece—for the NAC, the nursing staff, and the entire IDT—that should have occurred along with these definition changes often did not take place. Your team, starting with the NAC, needs to understand what the definitions mean, and frontline nursing and therapy staff should be documenting falls using these revised definitions. That’s the first step to achieve accurate MDS coding.”
Promote an interdisciplinary approach to coding decisions
The takeaway for the DNS is that the IDT has a key role to play in falls reporting on the MDS, suggests Szumlinski. “At the end of the day, CMS is looking for consistency and credibility between the nursing and therapy documentation in the nursing home—and also with documentation from the hospital if the resident is sent out. So, you need to have an IDT process that uses these updated falls definitions to come to a consensus clinical judgment about the MDS coding.”
The IDT—not the NAC alone—should review the documentation and discuss each incident, explains Szumlinski. “The team needs to determine whether the incident meets the definition of a fall. If it does and the resident was injured, the team then must decide: Is this a minor injury (i.e., an injury (except major)), or is this a major injury? The process that the IDT used to come to a consensus and the rationale for their decision should be documented in the medical record for each resident who has a fall-related incident.”
Szumlinski offers the following excerpt from HeathCap’s tool Understanding the 2025 MDS 3.0 Changes: Falls And Injuries to summarize the IDT’s role in determining whether an injury qualifies as injury (except major) or major injury:
Work with the hospital to get timely documentation
Obtaining the appropriate hospital documentation is critical to coding J1900 accurately when the resident is sent to the hospital following a fall, stresses Szumlinski. “Needing to send the resident to the hospital does not mean that the resident necessarily has a major injury, but many major injuries, such as subdural hematomas, will only be diagnosed at the hospital.”
All nursing homes should have a process for obtaining hospital documentation about resident falls that occurred during the look-back period before the assessment reference date (ARD) of the MDS assessment, says Szumlinski. “This will help the IDT conduct a thorough incident review and make an accurate coding decision about the type of injury.”
That process also needs to include an IDT review of any falls documentation that the hospital provides after the ARD, says Szumlinski. “If the team determines that a coding change is required for a submitted MDS (e.g., a fall that was classified as injury (except major) should be reclassified as major injury), the NAC must make a modification to that MDS assessment. The coding instructions in the RAI User’s Manual (pages J-39 – J-40 in chapter 3) make this very clear.”
Start with improving fall risk assessments to finetune fall prevention
Some nursing homes may need to improve their fall prevention programs as a result of these changes, notes Szumlinski. “In many facilities, that will mean changing how you do things more than what you do.”
Szumlinski offers the example of a newly admitted resident. “Nursing staff at every nursing home do a fall risk assessment at admission so that the facility can implement the required resident-centered fall prevention plan for residents who are at risk for a fall or who have a history of falls.”
However, changing how that admission fall risk assessment is conducted can improve the identification of fall risks, suggests Szumlinski. “Instead of doing a single fall risk assessment when a resident first comes in the door, it can be beneficial to do a fall risk assessment on every shift for the first three days of the resident’s stay, especially when they already have an identified risk at admission.”
The concern is that the resident is not a static person, points out Szumlinski. “You are looking at someone who is pretty dynamic. For example, the resident may not exhibit much of a fall risk at 1 p.m. when nursing staff do the initial fall risk assessment, but at 8 p.m., they may be sundowning and wobbly. Then at midnight, they may have taken a diuretic, and they get up to use the bathroom by themselves without the call light because they are confused. So, that 72-hour window of fall risk assessments will help you identify different levels of risk at different times of day.”
Conducting nine fall risk assessments instead of one for a new admission isn’t easy to do, acknowledges Szumlinski. “They take more staff time. Ultimately, however, you will get a much better picture of the resident assessing them that way, allowing you to create a stronger fall prevention plan that is more tailored to the individual resident’s risk profile.”
Prioritize major injury prevention over fall prevention when warranted
Another step toward improving the facility’s fall prevention program involves shifting the IDT’s focus from fall prevention to major injury prevention for some residents, says Szumlinski. “In Appendix PP of the State Operations Manual, CMS acknowledges that not all falls or other adverse events are preventable. Some residents will fall no matter what fall prevention interventions are in place. In this scenario, you need to shift your focus to address, ‘Knowing that this resident may fall, how can we protect them to prevent a major injury?’”
Interventions to prevent major injury are often common-sense approaches, says Szumlinski. “For example, you have a resident who is at high risk of falls getting out of bed, so you put them in a low bed and appropriately place a mat for them to fall on. However, the nightstand remains at the head of the bed.”
In this scenario, a nightstand offers more risk than benefit, points out Szumlinski. “First, it’s not helpful to the resident as a functional table because they can’t reach the top of the nightstand from the low bed. Second, many residents will try to pull themselves up using the nightstand after they roll onto the mat. If the nightstand tips over, they are at much greater risk of a major injury.”
Similarly, an over-the-bed table often is left in the room of the resident who is on a low bed, says Szumlinski. The resident can’t use it as a table, but sometimes they will climb up it and use it as a walker, which also increases their risk of major injury. So, any equipment that is not being used and can increase the resident’s risk of a major injury should be stored safely away from the resident.”
Train staff to identify and report change in condition
“There is no magic in fall prevention,” says Szumlinski. “It starts with keeping your team aware of the residents. If a resident has a clinical change in status, you can be sure that resident is at higher risk for a fall.”
Implementing some type of Stop and Watch Early Warning Tool to identify early changes in condition can help reduce falls, says Szumlinski. “A resident having a change in condition that goes unnoticed until it’s really advanced is a common problem. Giving staff the training and resources that they need to help the residents is often more useful to prevent falls than extensive policy changes.”
Staff should be trained to be alert to changes in a resident, says Szumlinski. “I always tell people ‘if in doubt, write it out’ because even a subtle change may flag you that the resident is at higher risk for a fall. For example, your resident George always eats two desserts. But today, he doesn’t eat his first dessert or ask for the second. The change could be that subtle in the beginning, so your staff need to know the residents to be able to identify it.”
Reporting changes goes hand in hand with identifying changes, says Szumlinski. “Staff need to prioritize reporting. All too often when a negative outcome (e.g., a fall) occurs four or five days after the first sign of a change in condition, staff who are interviewed reveal that they knew about that early sign. Going back to the example of George, they might say, ‘I saw that George wasn’t eating any dessert when he always eats two servings. I encouraged him to eat his dessert, but no, I didn’t report it.’”
Note: For more information on how to improve a nursing home’s fall prevention program, review the April 2026 Clinical Practice Guideline on Falls and Fall Prevention in the Post-Acute and Long-Term Care Setting from the Post-Acute and Long-Term Care Medical Association (PALTmed).
Sources: Long-Stay Nursing Home—Falls With Major Injury Re-specification Technical Specification Report, Skilled Nursing Facility—Falls With Major Injury Re-specification Technical Specification Report, SNF QRP Measure Calculations and Reporting User’s Manual, MDS 3.0 Quality Measures User’s Manual, and chapter 4 of the Long-Term Care Facility Resident Assessment Instrument 3.0 User’s Manual (RAI User’s Manual).
Solve the Puzzle: How QMs Using Falls MDS Data Fit Into SNF QRP, SNF VBP, and NHQI/Five-Star
| Measure | FY 2026 (Oct. 1, 2025 – Sept. 30, 2026) | FY 2027 (Oct. 1, 2026 – Sept. 30, 2027) | FY 2028 (Oct. 1, 2027 – Sept. 30, 2028) | NHQI QM Used in Five-Star | |||
| SNF QRP | SNF VBP | SNF QRP | SNF VBP | SNF QRP | SNF VBP | ||
| Percent of Residents Experiencing One or More Falls With Major Injury (Long-Stay)* | No | No | No | Yes First performance period: FY 2025 (Oct. 1, 2024 – Sept. 30, 2025) First baseline period: FY 2023 (Oct. 1, 2022 – Sept. 30, 2023) Performance period case minimum: 20 residents | No | Yes Performance period: FY 2026 (Oct. 1, 2025 – Sept. 30, 2026) Baseline period: FY 2024 (Oct. 1, 2023 – Sept. 30, 2024) Performance period case minimum: 20 residents | Yes |
| Application of Percent of Residents Experiencing One or More Falls With Major Injury (Long-Stay)* | Yes | No | Yes J1900C counts toward MDS data submission threshold | No | Yes J1900C counts toward MDS data submission threshold | No | No |
| Discharge Mobility Score | Yes | No | Yes | No | Yes | No | No |
| Discharge Function Score | Yes | No | Yes | Yes First performance period: FY 2025 (Oct. 1, 2024 – Sept. 30, 2025) First baseline period: FY 2023 (Oct. 1, 2022 – Sept. 30, 2023) Performance period case minimum: 20 eligible stays | Yes | Yes Performance period: FY 2026 (Oct. 1, 2025 – Sept. 30, 2026) Baseline period: FY 2024 (Oct. 1, 2023 – Sept. 30, 2024) Performance period case minimum: 20 eligible stays | Yes |
* CMS is gearing up to replace these measures with the Respecified Hybrid Falls With Major Injury (FMI) Long-Stay Version in NHQI/Five-Star and the SNF VBP and the Respecified Hybrid FMI SNF Version in the SNF QRP. At press time, the switchover dates have not been announced.
Note: Prevalence of Falls (Long-Stay) is a state surveyor measure that is not publicly reported and is not included in this chart. However, it is now used by state surveyors to help select Special Focus Facilities, according to a Jan. 28, 2026, CMS memo.
Sources: The SNF QRP Measures and Technical Information page, the SNF VBP Measures page, and the Nursing Home Five-Star Quality Rating System Technical Users’ Guide.
This AAPACN resource is copyright protected. AAPACN individual members may download or print one copy for use within their facility only. AAPACN facility organizational members have unlimited use only within facilities included in their organizational membership. Violation of AAPACN copyright may result in membership termination and loss of all AAPACN certification credentials. Learn more.